Benchmark
Walking "heel-to-toe" without falling over and without assistance: one step or less.
September 2011 - IV
My treatment began in early September 2011 after over 3 weeks as an in-patient at the
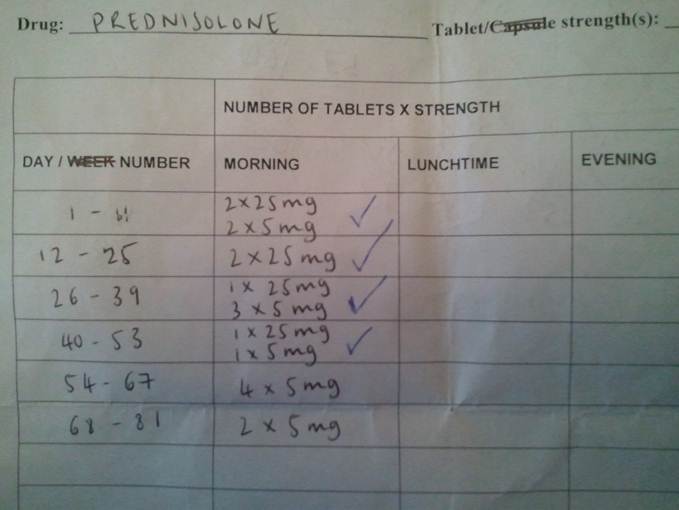
NHNN and came as a relief after a much longer that expected period of investigation. I was started on 1g/day of
prednisolone delivered intravenously for 5 days for an hour a day. This is a fairly common treatment strategy for CLIPPERS and
corticosteroids (like prednisolone) are often used to treat inflammatory disorders in brain and elsewhere. I improved during the IV treatment but not miraculously so. My facial numbness resolved, my walking became more fluid but my slow speech did return to normal. (In fact for a couple of days my speech went into over-drive and I couldn't be shut-up!). There was no change in my double vision and I still had numb fingers and tightness around my midriff. I also developed a tightness in my lower arms, especially on the right side. Additionally I developed "glitches" where my limbs would stiffen and I would walk like a tin-soldier for a few seconds if I was distracted or starting a new activity (e.g. walking somewhere after sitting down for a while). My speech would stall in a similar fashion - the words were queued up and ready to go but I couldn't get them out. These glitches were often accompanied by brief rushes of light-headedness. Over-all though, some modest improvement and a follow-up MRI two days after the end of the IV confirmed reduction in lesion appearance. So I was discharged and continued treatment at home. Note that this was another diagnostic hurdle - no improvement either in symptoms or in MRI would have meant that I wasn't "Responsive to Steroids" and therefore probably not CLIPPERS.